Spine Care
Infections: Tuberculosis of the Spine and Pyogenic
Overview
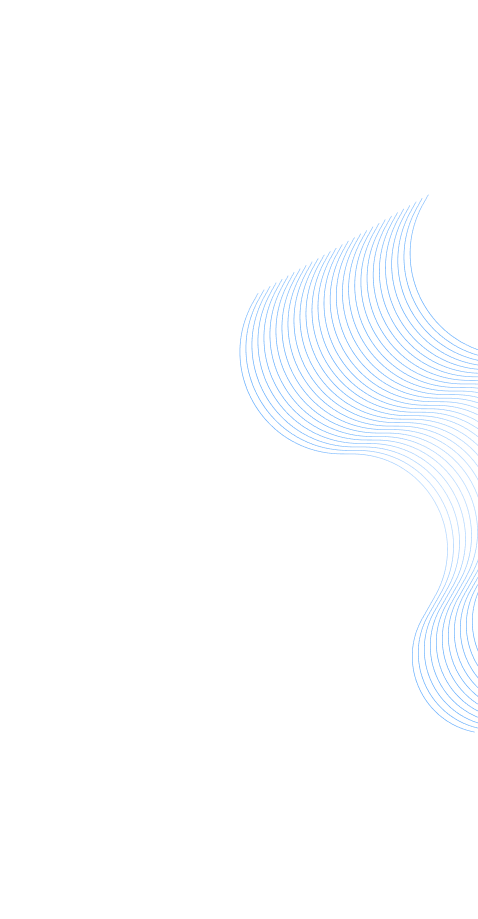
What is Spondylodiscitis?
It is characterized by invasion of Intervertebral disc and adjacent bone (vertebrae) by pathogens and formation of pus and reactive materials, causing destruction of the bone and disc tissue. Due to this there may be compression on the Spinal Cord/ Nerve roots causing weakness in the limbs or may lead to unstable spine with Severe pain.
How does Spondylodiscitis happen?
Spinal infections can be caused by either a bacterial or Fungal or Tubercular infection. Pathogens can infect the spine via three routes:
What are the common pathogens Causing infection in Indian population?
What are the common sites of Spondylodiscitis?
Are there risk factores for Spondylodiscitis?
What are the presenting symptoms?
Diagnosis of Spondylodiscitis
Diagnosis is based on clinical, laboratory and radiological features. It is often delayed or missed due to slow onset of symptoms and the high frequency of low back pain in the general population.
Laboratory Tests
Imaging Tools:
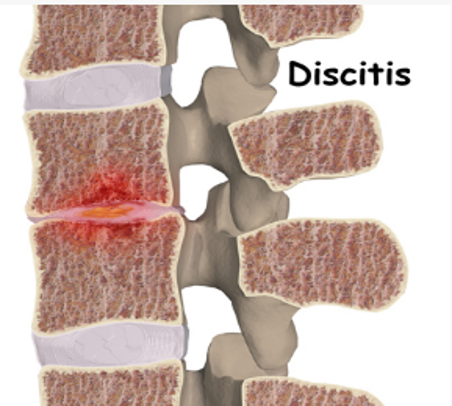
X-ray: Basic investigation to assess the bony anatomy.
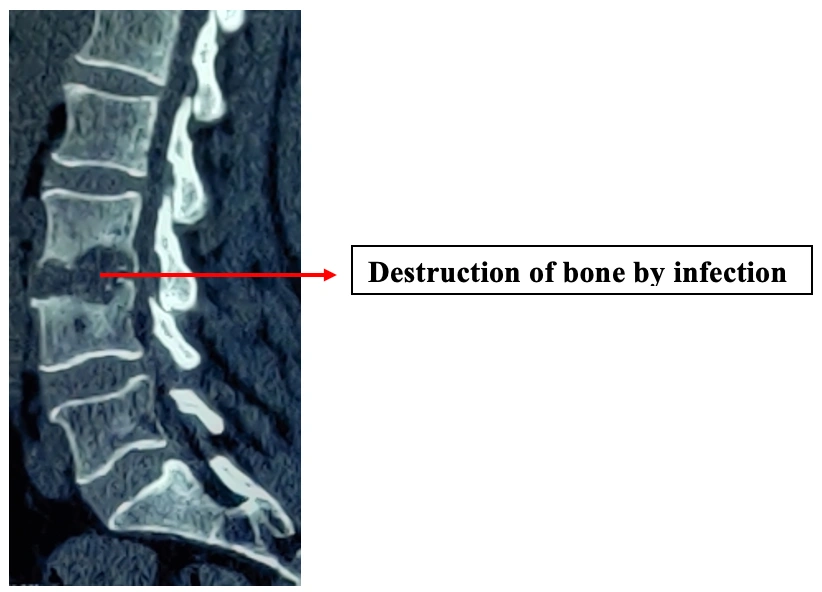
Destruction of disc and vertebral body
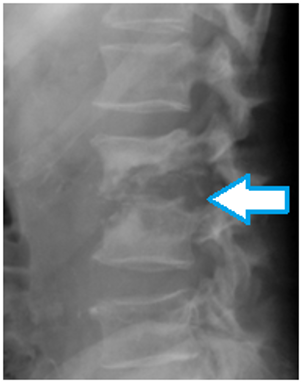
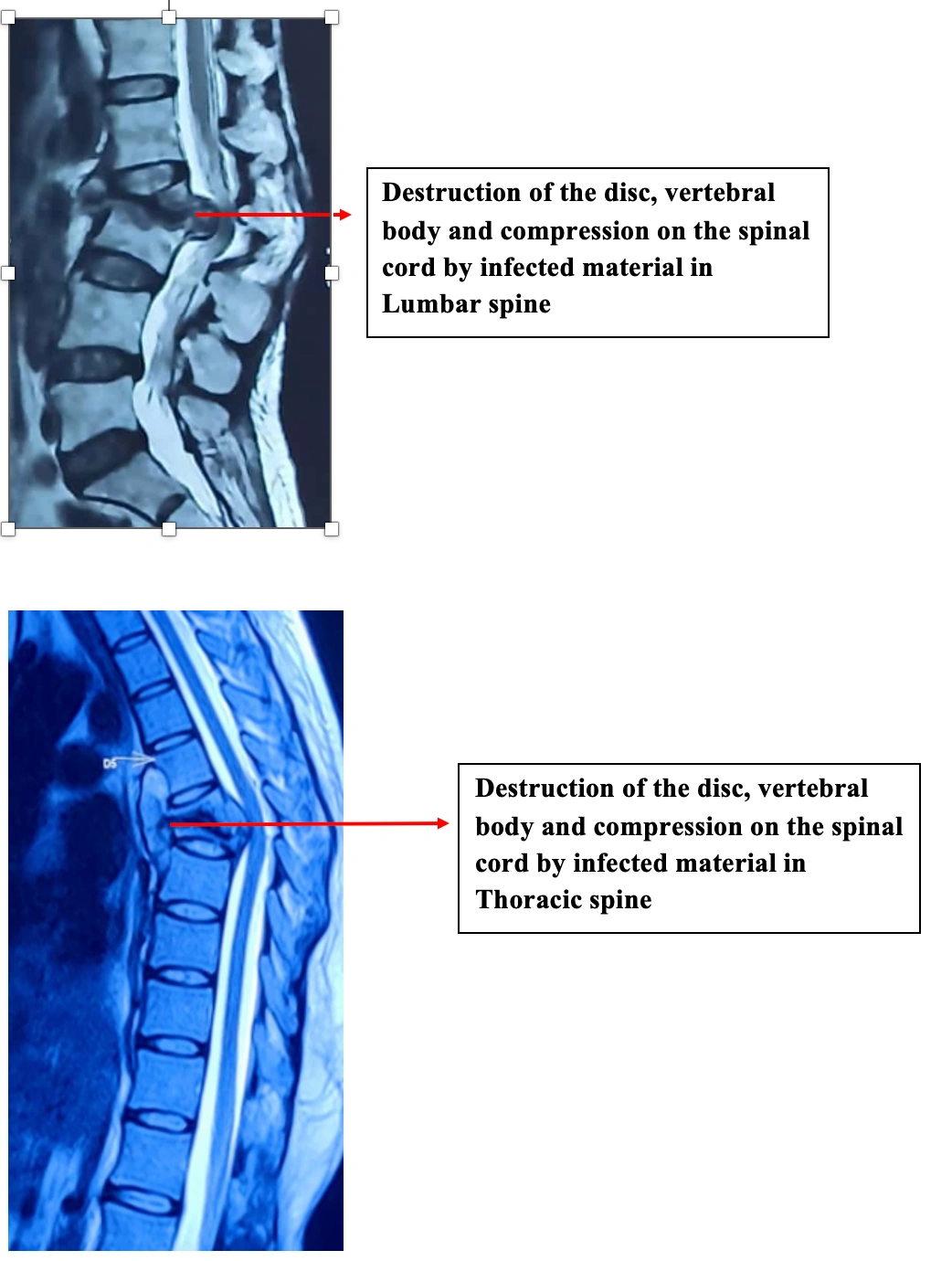
MRI: Investigation of choice. It allows for visualization of the soft tissues that include the nerves, spinal cord, and muscles of back and adjacent soft tissue around the spinal column.
CT Scan: Assessment of degree of bone destruction, Spinal instability and deformities if present.
Treatment:
Non Surgical: This option is viable for patients without spinal instability due to bony destruction and weakness in the limbs. It includes Injections or tablets (antibiotic/antifungal/ anti-tubercular therapy) for a prolonged duration.
Surgical:
Indications:
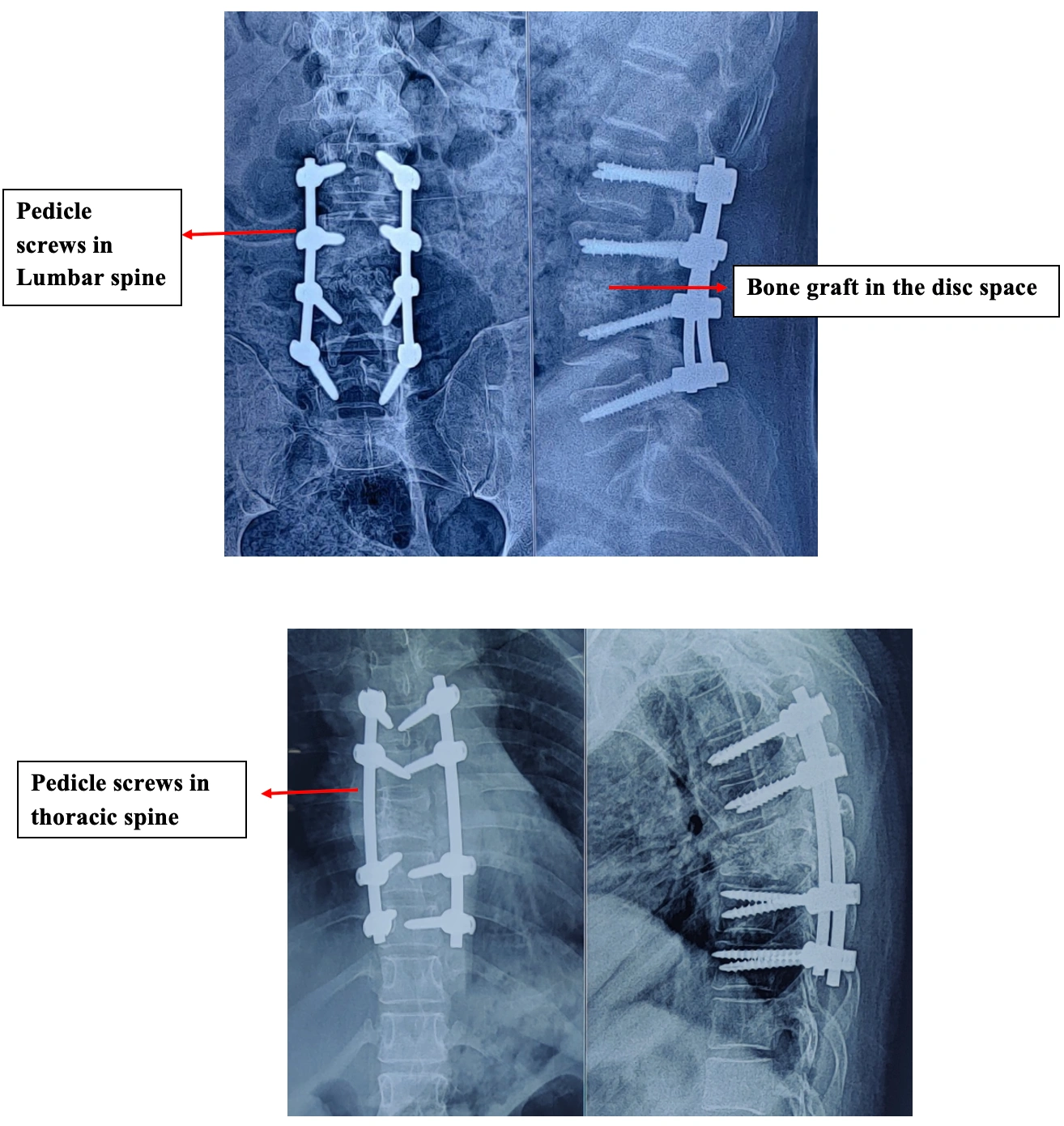
Stabilization by insertion of pedicle screw + Decompression of cord and nerve root by removal of Part of back bone and infected tissue+ Biopsy from the infected tissue + Filling of bone graft and antibiotics into the infected area/ insertion of cage.
Sample obtained from the affected area is sent for culture to grow the organism and sensitivity to the antibiotics is assessed. Sample is also sent for examination under microscope.
Possible complications:
It is characterized by invasion of Intervertebral disc and adjacent bone (vertebrae) by pathogens and formation of pus and reactive materials, causing destruction of the bone and disc tissue. Due to this there may be compression on the Spinal Cord/ Nerve roots causing weakness in the limbs or may lead to unstable spine with Severe pain.
How does Spondylodiscitis happen?
Spinal infections can be caused by either a bacterial or Fungal or Tubercular infection. Pathogens can infect the spine via three routes:
- Spread via Blood allowing seeding of infection from distant sites onto back bone.
- Direct external inoculationcommonly following spinal surgery, lumbar puncture or epidural procedures.
- Spread from contiguous tissues
What are the common pathogens Causing infection in Indian population?
- Bacteria: staphylococcus aureus, Escherichia coli
- Mycobacterium Tuberculosis, Brucellosis.
- Fungus: Candida, Aspergillosis
What are the common sites of Spondylodiscitis?
- Pyogenic spondylodiscitis affects preferentially the lumbar spine, followed by the thoracic and cervical spine in decreasing frequency (58%, 30% and 11% respectively).
- Tuberculosis (TB) lesions more commonly affect the thoracolumbar spine and less common in Cervical, Lumbosacral and in Craniovertebral junction
Are there risk factores for Spondylodiscitis?
- Old age,
- Diabetes Mellitus,
- Kidney and Liver diseases
- Previous infections: Skin, Urinary tract and dental infections.
- HIV
- IV drug addicts
What are the presenting symptoms?
- Symptoms vary depending on the type of spinal infection but, generally pain is localized initially at the site of the infection with or without radiation to the limbs..
- Fever, chills, rigors
- Reduced sleep due to night pain
- Weakness in the limbs, associated with difficulty in walking.
- Pus discharge (rare)
Diagnosis of Spondylodiscitis
Diagnosis is based on clinical, laboratory and radiological features. It is often delayed or missed due to slow onset of symptoms and the high frequency of low back pain in the general population.
Laboratory Tests
- Complete blood count(CBC)
- Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
- Blood culture
Imaging Tools:
X-ray: Basic investigation to assess the bony anatomy.
Destruction of disc and vertebral body
MRI: Investigation of choice. It allows for visualization of the soft tissues that include the nerves, spinal cord, and muscles of back and adjacent soft tissue around the spinal column.
CT Scan: Assessment of degree of bone destruction, Spinal instability and deformities if present.
Treatment:
Non Surgical: This option is viable for patients without spinal instability due to bony destruction and weakness in the limbs. It includes Injections or tablets (antibiotic/antifungal/ anti-tubercular therapy) for a prolonged duration.
Surgical:
Indications:
- Significant bone destruction causing spinal instability
- Weakness of the limbs.
- Spread of infection to blood with clinical toxicity caused by an abscess unresponsive to antibiotics.
- Failure of needle biopsy to obtain the needed cultures.
- Failure of non surgical mode of treatment.
Stabilization by insertion of pedicle screw + Decompression of cord and nerve root by removal of Part of back bone and infected tissue+ Biopsy from the infected tissue + Filling of bone graft and antibiotics into the infected area/ insertion of cage.
Sample obtained from the affected area is sent for culture to grow the organism and sensitivity to the antibiotics is assessed. Sample is also sent for examination under microscope.
Possible complications:
- Infection
- Weakness in the limbs
- Wound healing problems
- Need for secondary surgery